Subtotal ¥0.00
Learn Mass Casualty Incident Protocols for faster emergency response and accurate patient identification
The Foundation: Incident Command System (ICS) Structure
How do we manage the unmanageable? When a disaster strikes, the difference between a controlled response and total anarchy is the organizational framework we deploy immediately. As someone deeply invested in emergency solutions, I know that Mass Casualty Incident Protocols: Emergency Response and Patient Identification cannot function without a solid foundation. That foundation is the Incident Command System (ICS).
Unified Command and NIMS-Compliant Operations
In a crisis, jurisdictional boundaries blur. We rely on NIMS compliance (National Incident Management System) to ensure that fire, police, EMS, and hospital teams speak the same operational language. A Unified Command structure eliminates the “who is in charge?” confusion, allowing multiple agencies to work as a single, cohesive unit. This standardization is critical for scaling operations from a local traffic accident to a major regional disaster.
Key Roles: Triage, Transport, and Treatment Officers
To prevent bottlenecks, the ICS divides the Medical Branch into distinct functional areas. I always emphasize that success lies in strict role adherence:
- Triage Unit Leader: The first line of defense. They oversee the initial sorting of patients using the START triage algorithm, ensuring resources go where they are needed most.
- Treatment Unit Leader: Manages the casualty collection point, overseeing stabilization and re-triage before movement.
- Transport Unit Leader: The logistics hub. They coordinate ambulance ingress/egress and communicate with hospitals to manage surge capacity.
Communication Channels and Interoperability
The days of relying solely on chaotic radio traffic are fading. Effective response now requires interoperability between voice comms and digital data. When a patient is tagged—ideally with a durable, weather-resistant identifier like the solutions we engineer at LinkWin—that data point must travel instantly. Integrating patient tracking systems with traditional radio reports ensures that the Incident Commander has real-time visibility, reducing the risk of losing track of patients during the “fog of war.”
Phase One: Triage Protocols and Categorization
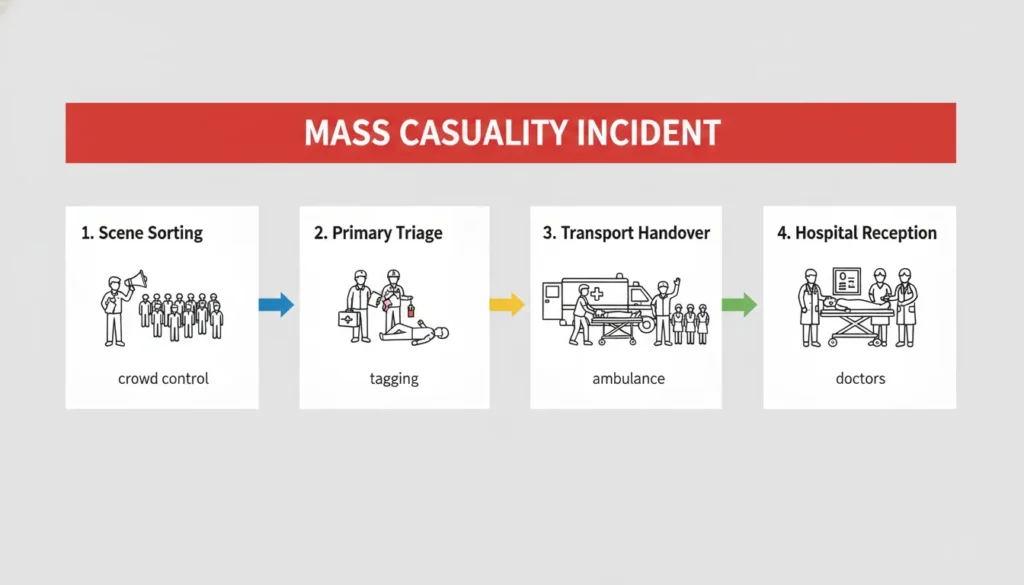
In the initial moments of a crisis, speed is absolute. We implement Mass Casualty Incident Protocols to bring immediate order to chaos. The first step isn’t treatment; it is sorting. We have to make tough calls instantly to save the most lives, and that requires a rigid, disciplined approach to categorization.
Primary Triage: START, JumpSTART, and SALT Algorithms
When we arrive on the scene, we rely on established algorithms to categorize patients rapidly. The START triage algorithm (Simple Triage and Rapid Treatment) remains the gold standard for adults. It focuses strictly on ability to walk, breathing, and circulation. For children, we switch to JumpSTART to account for physiological differences. Recently, the SALT (Sort, Assess, Lifesaving Interventions, Treatment/Transport) method has gained traction for its comprehensive approach to mass casualty trauma care.
- Red (Immediate): Critical condition requiring immediate intervention.
- Yellow (Delayed): Serious injuries but currently stable.
- Green (Minor): The “walking wounded” who can move on their own.
- Black (Deceased/Expectant): No hope for survival given the current resources.
Secondary Triage at the Casualty Collection Point
Initial assessments are just a snapshot in time. Once patients are moved to the casualty collection point, we conduct secondary triage. A patient initially marked “Yellow” might deteriorate into “Red,” or we might find that additional resources allow us to treat an “Expectant” patient. This continuous re-evaluation ensures that emergency medical services (EMS) protocols remain dynamic and responsive to the shifting reality of the disaster.
The “Tagging” Ritual: Why Standard Paper Tags Fail
Here is where I see the biggest operational failure. We rely on triage tags color coding to visually communicate patient status, but standard paper tags are a massive liability. In the field, we deal with rain, mud, bodily fluids, and rough handling.
- Weather Vulnerability: Standard paper dissolves in rain or snow, erasing vital data instantly.
- Physical Tearing: Flimsy strings snap during transport, leaving patients unidentified.
- Illegibility: Handwritten notes smear and become unreadable in wet conditions.
If the tag fails, the patient tracking system breaks down before it even starts. We need durable, synthetic materials that withstand the elements, ensuring that the identity and status we assign in the field stick with the patient all the way to the hospital.
The Core Challenge: Patient Identification in Crisis
In my experience, the hardest part of Mass Casualty Incident Protocols: Emergency Response and Patient Identification isn’t just the medical treatment; it’s knowing exactly who is who. When we are dealing with mass casualty trauma care, we often face the “John Doe” problem. Victims are unconscious, in shock, or stripped of personal effects, making immediate identification impossible. We cannot wait for a wallet check; we need to track that patient the second we find them.
Establishing the Chain of Identity
To manage this, we have to build a Chain of Identity immediately. We don’t wait for a legal name. Instead, we assign a unique Temporary ID using physical identifiers like RFID patient wristbands or barcoded tags. This links the patient to their clinical data from the moment they are processed at the casualty collection point. This association ensures that even if a patient is moved, their medical record moves with them.
Common Pitfalls in Manual Tracking
Relying on old-school methods during a surge often leads to data disasters. Without a solid patient tracking system, here is where I see the process break down:
- Duplicate Numbering: Different triage teams accidentally assign the same ID number to different victims, causing dangerous confusion.
- Lost Wristbands: Low-quality bands tear or fall off during transport, destroying the link needed for victim reunification.
- Illegible Handwriting: In bad weather or high stress, markers smear and handwriting becomes unreadable, rendering the tag useless.
Bridging the Gap: From Ambulance to Hospital Admission
The transition from the chaos of the field to the clinical environment of a hospital is often where the chain of survival breaks. If we don’t manage this handoff correctly, the organization established at the scene falls apart the moment the ambulance doors open. Effective Mass Casualty Incident Protocols: Emergency Response and Patient Identification must extend seamlessly beyond the transport phase.
Pre-Arrival Notification
We cannot simply show up at the emergency bay with critical patients unannounced. Hospitals need lead time to prepare. We rely on ePCR (Electronic Patient Care Reporting) and radio systems to transmit data before the wheels stop rolling.
- Data Transmission: By scanning a barcode on the field tag, we send vital signs and injury codes directly to the receiving facility.
- Resource Activation: This early warning allows the facility to activate its Hospital emergency operations plan (EOP), ensuring trauma surgeons and operating rooms are prepped for specific injuries.
Hospital Surge Protocols and Rapid Registration
When multiple units arrive simultaneously, the standard intake desk becomes a bottleneck. To prevent a logjam, we implement surge capacity management strategies immediately. This often involves setting up external triage tents outside the main entrance to re-evaluate patients.
We bypass the usual administrative red tape. Instead of asking for insurance cards, admission teams use rapid registration protocols. They scan the RFID patient wristbands or barcodes applied in the field to create a temporary “John Doe” medical record. This ensures the patient is in the system within seconds, allowing medical staff to focus on mass casualty trauma care rather than paperwork.
Continuity of Care
The most dangerous gap in this phase is the loss of treatment history. If a paramedic administers morphine or applies a tourniquet in the field, the ER doctor must know immediately. We have to link field medication records to the hospital’s internal system.
By maintaining this digital thread, we ensure continuity of care. The patient’s unique ID ties their pre-hospital treatment to their in-hospital chart, preventing medication errors and ensuring that the treatment plan is based on the full picture, not just what is seen in the trauma bay.
Modern Technology in MCI Management
When we look at evolving Mass Casualty Incident Protocols: Emergency Response and Patient Identification, the shift from analog to digital isn’t just a luxury; it is a necessity. I have seen chaotic scenes where paper tags turn into pulp in the rain, losing critical patient data instantly. Modern tech solves this by replacing fragile paper with robust digital solutions that ensure data integrity during a crisis.
Digital Triage Systems vs. Paper Tags
The debate between handheld scanners and traditional paper is effectively over. Digital systems allow responders to input vital signs and injury severity directly into an ePCR (Electronic Patient Care Reporting) system within seconds.
- Speed: Scanners capture data significantly faster than writing by hand.
- Durability: Ruggedized devices withstand weather, mud, and blood, unlike standard cardstock.
- Accuracy: Eliminates the risk of illegible handwriting during high-stress moments.
RFID and Barcode Solutions
We are seeing a massive uptake in RFID patient wristbands and barcode technology. These tools drastically reduce human error. Instead of manually transcribing numbers, a quick scan links the victim to their medical record immediately. This automation ensures that the Mass Casualty Incident Protocols: Emergency Response and Patient Identification remain watertight from the field to the hospital, preventing identity mix-ups.
Real-Time Patient Tracking Dashboards
For the Incident Commander, visibility is everything. A robust patient tracking system feeds data into a central dashboard, offering a real-time view of the entire operation.
- Resource Allocation: See instantly which sector is overwhelmed and needs support.
- Transport Logic: Track exactly which ambulance is carrying which patient to prevent hospital bottlenecks.
- Status Updates: Monitor changes in triage categories live as patients move through the chain of care.
Training and Drills: Testing Our Mass Casualty Incident Protocols
Regular training and drills are non-negotiable for anyone involved in emergency response. We can design the most advanced MCI protocols and deploy cutting-edge patient tracking systems, but without rigorous testing, their real-world effectiveness remains unknown. Our approach ensures every team member, from the initial EMS protocols responders to hospital staff, is ready.
Tabletop Exercises: Simulating Data Flow
We kick things off with tabletop exercises. These aren’t just discussions; they’re critical simulations where we walk through the entire incident lifecycle, focusing heavily on data flow. We trace the journey of a patient’s identity and medical information from the moment of primary triage in the field through to hospital admission. This allows us to identify potential bottlenecks in our communication channels and pinpoint where patient identification might falter before an actual crisis hits. It’s about ensuring everyone understands the importance of precise data management and how information moves within the Incident Command System (ICS) structure.
Full-Scale Drills: Testing Durability and Speed
Beyond the table, we conduct extensive full-scale drills. These are crucial for testing the physical and practical aspects of our MCI protocols. We deploy our teams to simulate realistic scenarios, assessing everything from the speed of START triage algorithm application to the efficiency of setting up casualty collection points. A key focus during these disaster preparedness drills is the durability of our RFID patient wristbands and other temporary ID solutions. We test how quickly our digital triage systems can scan and process patient data, looking for any slowdowns or points of failure. This also allows us to evaluate our surge capacity management and the initial steps of hospital emergency operations plan (EOP) activation under pressure.
Post-Incident Analysis: Refining Identification Protocols
Every drill concludes with a thorough post-incident analysis. This isn’t about assigning blame; it’s about continuous improvement. We meticulously review all aspects of the response, with a particular emphasis on any identification failures. Did a triage tag get lost? Was an RFID patient wristband unreadable? Were there issues with duplicate numbering or data transfer from ePCR to hospital systems? By dissecting these challenges, we gather invaluable insights that allow us to refine our patient identification strategies, update our MCI protocols, and strengthen the resilience of our entire emergency response framework.
